Summary:
COPD 2017 conference is a three-day program of presentations, panel discussions and interactive dialogue at the conference on leading the way in the COPD research and development, which will be held during May 29-31,2017 in Osaka, Japan. The event brings together Professors, researchers,key officials and delegates from almost 50 countries to review the role in the COPD management and engage in interactive talks,sessions,workshops in the current recent advancements in COPD strategies.
Importance & Scope:
Chronic obstructive pulmonary disease (COPD) is an important public health issue in many countries which is estimated to become the fifth cause of disability and the third cause of mortality in the world by 2020. Educating patients and physicians to recognize that cough, sputum production, and especially breathlessness are not trivial symptoms is an essential aspect of the public health care of this disease. This landmark study forms an additional foundation for the early history of smoking in order to identify abnormality and risk of progressive impairment on the pathway to symptomatic COPD.
Osaka is a designated city in the Kansai region of Japan. It is the capital city of Osaka Prefecture and the largest component of the Keihanshin Metropolitan Area, the second largest metropolitan area in Japan and among the largest in the world with over 19 million inhabitants. Osaka is situated at the mouth of the Yodo River on Osaka Bay, Japan. Osaka has started to garner more attention from foreigners with the increased popularity of cooking and dining in popular culture. Osaka Science Museum is in a five storied building next to the National Museum of Art, with a planetarium and an OMNIMAX theatre. The Museum of Oriental Ceramics holds more than 2,000 pieces of ceramics, from China, Korea, Japan and Vietnam, featuring displays of some of their Korean celadon under natural light.
Conference Highlights
Types of COPD
Signs and Symptoms of COPD
Pathogenesis of COPD
Pathophysiology of COPD
Management of COPD
COPD Complications
Co-Morbidities in COPD
Epidemiology of COPD
Diagnostic Evaluation of COPD
COPD Therapeutics
COPD Exacerbations
Self-Management and Prevention of COPD
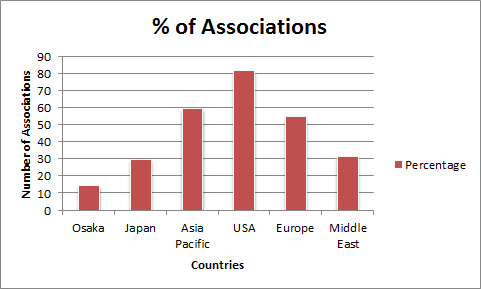
Major COPD Research Associations around the Globe
Alpha-1 Foundation
American Association for Respiratory Care
American College of Chest Physicians
American College of Emergency Physicians
American College of Physicians
American Lung Association
Asian Pacific Society of Respirology
Associacion Argentina de Medicina Respiratoria
Association of Bulgarians with Bronchial Asthma (ABBA)
Canadian Lung Association (CLA)
Chinese COPD Patient Education Organziation
COPD Club of Northern Thailand
COPD Foundation
COPD Patient Organization of Vietnam
COPD Patients Club Kyrgyzstan
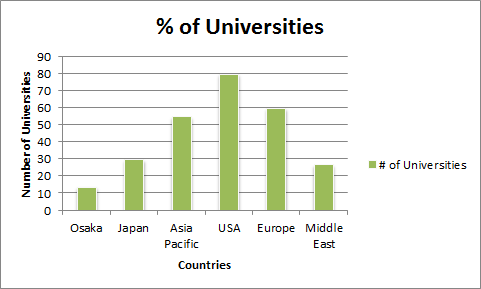
Major Universities on COPD Research
Australian national university, Australia
Charles Darwin University Casoria Australia
Columbia University Medical Center, United States
Curtin University Bentley, Australia
Dar Al Uloom University, Saudi Arabia
Harvard University, United States
Imperial College London, United Kingdom
Iqbal Chest Centre, Bangladesh
Kumamoto University, Japan
Linnaeus University, Sweden
Macquarie University, Australia
Mayo Clinic College of Medicine, USA
McGill university Montréal, Canada
Medi7 Bentleigh, Australia
University Of California Los Angeles, United States
Companies Associated with COPD Research
Almirall, Spain
Amphastar Pharmaceuticals, Inc
AstraZeneca, Switzerland
Bayer, Germany
Beacon Pharmaceuticals
Biotie Therapies Corp
Bioxyne Limited
Boehringer Ingelheim, Germany
Chiesi Pharmaceutical, Italy
Cohero Health
Forest Laboratories, USA
Gecko Health, USA
Gsk, London
Panmira Pharmaceuticals, LLC
Pearl Therapeutics, Inc
PT Boehringer Ingelheim Indonesia
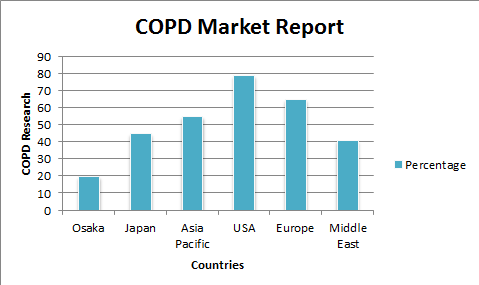
Market Research
COPD market is estimated to currently be worth $11.3 billion, and is forecast to reach a value of $15.6 billion by 2019. Much of this growth will be fuelled by a high number of new, more efficacious and convenient products entering the market and commanding greater value compared to the therapies already in the market. The drugs driving this growth include once-daily LABA/LAMA fixed-dose combinations such as QVA-149, umeclidinium bromide/vilanterol and olodaterol/tiotropium. The asthma and COPD Therapies Market 2015-2025 report examines the current and future pharmaceutical treatments for these two respiratory diseases.With reported numbers for both asthma and COPD showing growth all over the world, understanding the market and the treatments available is crucial for all those in fields related to the sector. Currently, North America leads the global market for asthma & COPD drugs and devices. North America was followed by Europe in terms of market capitalization. However, North America and Europe is expected to lose out some of the market share to other emerging regional markets owing to the expiry of several patens of pharmaceutical companies operating in these regions. Asia Pacific is expected to be the fastest regional market for asthma and COPD owing to the increased incidence of asthma & other respiratory diseases in industrial regions.
Chronic Obstructive Pulmonary Disease is characterized by obstruction of the airways and limitation to airflow. People with COPD have trouble breathing and shortness of breath.
The diseases that fall under the scope of COPD are: Chronic Bronchitis, Emphysema and COPD-Asthma overlap. Chronic Bronchitis causes inflammation and irritation of the airways, the tubes in your lungs where air passes through. When the air tubes are inflamed and irritated, thick mucus begins to form in them. Over time, this mucus plugs up airways and makes breathing difficult. When you cough this mucus up, the excretions are known as sputum, or phlegm. Emphysema is a common type of COPD in which the air sacs of the lungs become damaged, causing them to enlarge and burst. Damage in this area makes it difficult for people with emphysema to expel air from their lungs. This leads to a build-up of carbon dioxide in the body and a myriad of emphysema signs and symptoms. Asthma COPD Overlap Syndrome (ACOS) is usually characterized by increased reversibility of airflow obstruction, eosinophilic bronchial and systemic inflammation, and increased response to inhaled corticosteroids, compared with COPD patients. The relevance of the ACOS is the need to identify patients with COPD who may have underlying eosinophilic inflammation that responds better to inhaled corticosteroids. Until new diagnostic tools are developed, a previous diagnosis of asthma in a patient with COPD can be a reliable criterion to suspect ACOS in a patient with COPD.
Related Conference: 3rd Euro-Global Infectious Diseases Conferences September 5-6, 2016 Frankfurt, Germany; 3rd Euro-Global Emerging Infectious Diseases Conferences September 5-6, 2016 Frankfurt, Germany;4th Euro Global Conference on Infectious Diseases, October 16-18, 2017 Paris, France; 5th International Congress on Bacteriology and Infectious Diseases May 25-26, 2017 Chicago, USA; 2nd International Conference on Chest, March 24-26, 2017 Melbourne, Australia; 2nd International Conference on Respiratory and Pulmonary Medicine, August 6-8, 2017 London, UK; 3rd world Congress on Infectious Disease, August 28-30, Philadelphia, USA; International Conference on American Thoracic Society, May 19-24, 2017, USA; Malaysian Thoracic Society Annual Congress, 28–30 July 2016 Hyogo, Japan; 58th Annual Meeting of the Japan Lung Cancer Society 4–15 October 2017, Japan; World Sleep 2017 October 6-7, Prague, Czech Republic; Australian & New Zealand Society of Cardiac & Thoracic Surgeons Annual Scientific Meeting, 6–9 November 2016 Queensland, Australia
Track 2: Signs and Symptoms of COPD
COPD symptoms are classified into Typical and non-typical type, which includes Chronic Cough, wheezing and shortness of breath and fatigue associated with sputum productions and the amount of sputum produced can change over hours to days. Typically the shortness of breath is worse on exertion of a prolonged duration and worsens over time. In the advanced stages, it occurs during rest and may be always present. It is a source of both anxiety and a poor quality of life in those with COPD. Many people with more advanced COPD breathe through pursed lips and this action can improve shortness of breath in some. Non Typical symptoms associated with Haemoptysis which can occur due to COPD, and also continuous expectoration of purulent sputum along with breathlessness without productive cough or wheezing. Clinical Features leads to high pressure on the lung arteries, which strains the right ventricle of the heart. This situation is referred to as corpulmonale, and leads to symptoms of leg swelling and bulging neck veins. Those with obstructed airflow may have wheezing or decreased sounds with air entry on examination of the chest with a stethoscope. A barrel chest is a characteristic sign of COPD.
Related Conference: 3rd Euro-Global Infectious Diseases Conferences September 5-6, 2016 Frankfurt, Germany; 3rd Euro-Global Emerging Infectious Diseases Conferences September 5-6, 2016 Frankfurt, Germany; 5th International Congress on Bacteriology and Infectious Diseases May 25-26, 2017 Chicago, USA; 3rd world Congress on Infectious Disease, August 28-30, Philadelphia, USA; 2nd International Congress on Rare Diseases and Orphan Drugs, October 16-18, 2017 San Antonio, USA; 4th Euro Global Conference on Infectious Diseases, October 16-18, 2017 Paris, France; 2nd International Conference on Chest, March 24-26, 2017 Melbourne, Australia; World Sleep 2017 October 6-7, Prague, Czech Republic; 74th Annual Congress of the American College of Allergy, Asthma & Immunology (ACAAI) Oct 26-30, 2017 Boston, USA; 58th Annual Meeting of the Japan Lung Cancer Society 4–15 October 2017, Japan; 8th International Workshop on Pulmonary Functional Imaging 24–26 March 2017 Seoul, Korea; Better Breathing Conference Jan 26-28, 2017 Toronto, Canada
Track 3: Pathogenesis of COPD
The diseases that fall under the scope of COPD are: Chronic Bronchitis, Emphysema and COPD-Asthma overlap. Chronic Bronchitis causes inflammation and irritation of the airways, the tubes in your lungs where air passes through. When the air tubes are inflamed and irritated, thick mucus begins to form in them. Over time, this mucus plugs up airways and makes breathing difficult. When you cough this mucus up, the excretions are known as sputum, or phlegm. Emphysema is a common type of COPD in which the air sacs of the lungs become damaged, causing them to enlarge and burst. Damage in this area makes it difficult for people with emphysema to expel air from their lungs. This leads to a build-up of carbon dioxide in the body and a myriad of emphysema signs and symptoms. Asthma COPD Overlap Syndrome (ACOS) is usually characterized by increased reversibility of airflow obstruction, eosinophilic bronchial and systemic inflammation, and increased response to inhaled corticosteroids, compared with COPD patients. The relevance of the ACOS is the need to identify patients with COPD who may have underlying eosinophilic inflammation that responds better to inhaled corticosteroids. Until new diagnostic tools are developed, a previous diagnosis of asthma in a patient with COPD can be a reliable criterion to suspect ACOS in a patient with COPD.
Related Conference: 3rd Euro-Global Infectious Diseases Conferences September 5-6, 2016 Frankfurt, Germany; 3rd Euro-Global Emerging Infectious Diseases Conferences September 5-6, 2016 Frankfurt, Germany; 2nd International Conference on Respiratory and Pulmonary Medicine, August 6-8, 2017 London, UK; 3rd International Conference on Influenza, September 11-13, 2017 Zurich, Switzerland; International Conference on Pulmonary Disorders, April 20-21, 2017 Las Vegas, USA; 2nd International Conference on Chest, March 24-26, 2017 Melbourne, Australia; 4th Euro Global Conference on Infectious Diseases, October 16-18, 2017 Paris, France; International Conference on American Thoracic Society, May 19-24, 2017, USA; Malaysian Thoracic Society Annual Congress, 28–30 July 2016 Hyogo, Japan; Australian & New Zealand Society of Cardiac & Thoracic Surgeons Annual Scientific Meeting, 6–9 November 2016 Queensland, Australia; Better Breathing Conference Jan 26-28, 2017 Toronto, Canada; 8th International Workshop on Pulmonary Functional Imaging 24–26 March 2017 Seoul, Korea
Track 4: Pathophysiology of COPD
The diseases that fall under the scope of COPD are: Chronic Bronchitis, Emphysema and COPD-Asthma overlap. Chronic Bronchitis causes inflammation and irritation of the airways, the tubes in your lungs where air passes through. When the air tubes are inflamed and irritated, thick mucus begins to form in them. Over time, this mucus plugs up airways and makes breathing difficult. When you cough this mucus up, the excretions are known as sputum, or phlegm. Emphysema is a common type of COPD in which the air sacs of the lungs become damaged, causing them to enlarge and burst. Damage in this area makes it difficult for people with emphysema to expel air from their lungs. This leads to a build-up of carbon dioxide in the body and a myriad of emphysema signs and symptoms. Asthma COPD Overlap Syndrome (ACOS) is usually characterized by increased reversibility of airflow obstruction, eosinophilic bronchial and systemic inflammation, and increased response to inhaled corticosteroids, compared with COPD patients. The relevance of the ACOS is the need to identify patients with COPD who may have underlying eosinophilic inflammation that responds better to inhaled corticosteroids. Until new diagnostic tools are developed, a previous diagnosis of asthma in a patient with COPD can be a reliable criterion to suspect ACOS in a patient with COPD.
Related Conference: 3rd Euro-Global Infectious Diseases Conferences September 5-6, 2016 Frankfurt, Germany; 3rd Euro-Global Emerging Infectious Diseases Conferences September 5-6, 2016 Frankfurt, Germany; 5th International Congress on Bacteriology and Infectious Diseases May 25-26, 2017 Chicago, USA; International Conference on Pulmonary Disorders, April 20-21, 2017 Las Vegas, USA; 2nd International Conference on Chest, March 24-26, 2017 Melbourne, Australia; 3rd International Conference on Influenza, September 11-13, 2017 Zurich, Switzerland; 2nd International Conference on Respiratory and Pulmonary Medicine, August 6-8, 2017 London, UK
Track 6: Complications Associated with COPD
Chronic obstructive pulmonary disease (COPD) refers to a collection of lung diseases that can lead to blocked airways. People with COPD can be at risk for some serious complications that can not only put their health in jeopardy, but can also fatal. In COPD patients, Pneumonia occurs when bacteria enter the lungs, creating an infection. For COPD patients, pneumonia can weaken the lungs. This can lead to a chain reaction of illnesses that can weaken the lungs even further. This downward spiral can lead to a rapid deterioration of health in COPD patients. Respiratory Insufficiency is an important complication of chronic obstructive pulmonary disease. This may represent deterioration in the patient's premorbid condition such that hypoxemia worsens and hypercapnia develops during a relatively trivial respiratory tract infection, which may be viral or bacterial, Alternatively, these changes may occur for the first time in someone with less severe COPD who encounters a particularly dramatic cause for deterioration, e.g. lobar pneumonia or acute pulmonary oedema. Pneumothorax is defined as the accumulation of air or gas in the space between the lung and the chest wall. Also known as a collapsed lung, pneumothorax occurs when a hole develops in the lung that allows air to escape in the space around the lung, causing the lungs to partially or completely collapse. People with COPD, are at greater risk for pneumothorax because the structure of their lungs is weak and vulnerable to the spontaneous development of these types of holes. Pneumo mediastinum must be differentiated from spontaneous pneumothorax. Patients may or may not have symptoms, as this is typically a well-tolerated disease, although mortality in cases of esophageal rupture is very high.
Related Conference: 3rd Euro-Global Infectious Diseases Conferences September 5-6, 2016 Frankfurt, Germany; 3rd Euro-Global Emerging Infectious Diseases Conferences September 5-6, 2016 Frankfurt, Germany; 3rd world Congress on Infectious Disease, August 28-30, Philadelphia, USA; 4th Euro Global Conference on Infectious Diseases, October 16-18, 2017 Paris, France; International Conference on Pulmonary Disorders, April 20-21, 2017 Las Vegas, USA; 3rd International Conference on Influenza, September 11-13, 2017 Zurich, Switzerland; 2nd International Conference on Chest, March 24-26, 2017 Melbourne, Australia; International Conference on American Thoracic Society, May 19-24, 2017, USA; Australian & New Zealand Society of Cardiac & Thoracic Surgeons Annual Scientific Meeting, 6–9 November 2016 Queensland, Australia; 8th International Workshop on Pulmonary Functional Imaging 24–26 March 2017 Seoul, Korea; 74th Annual Congress of the American College of Allergy, Asthma & Immunology (ACAAI) Oct 26-30, 2017 Boston, USA; World Sleep 2017 October 6-7, Prague, Czech Republic
Track 7: CO-Morbidities in COPD
Chronic obstructive pulmonary disease (COPD) refers to a collection of lung diseases that can lead to blocked airways. People with COPD can be at risk for some serious complications that can not only put their health in jeopardy, but can also fatal. In COPD patients, Pneumonia occurs when bacteria enter the lungs, creating an infection. For COPD patients, pneumonia can weaken the lungs. This can lead to a chain reaction of illnesses that can weaken the lungs even further. This downward spiral can lead to a rapid deterioration of health in COPD patients. Respiratory Insufficiency is an important complication of chronic obstructive pulmonary disease. This may represent deterioration in the patient's premorbid condition such that hypoxemia worsens and hypercapnia develops during a relatively trivial respiratory tract infection, which may be viral or bacterial, Alternatively, these changes may occur for the first time in someone with less severe COPD who encounters a particularly dramatic cause for deterioration, e.g. lobar pneumonia or acute pulmonary oedema. Pneumothorax is defined as the accumulation of air or gas in the space between the lung and the chest wall. Also known as a collapsed lung, pneumothorax occurs when a hole develops in the lung that allows air to escape in the space around the lung, causing the lungs to partially or completely collapse. People with COPD, are at greater risk for pneumothorax because the structure of their lungs is weak and vulnerable to the spontaneous development of these types of holes. Pneumo mediastinum must be differentiated from spontaneous pneumothorax. Patients may or may not have symptoms, as this is typically a well-tolerated disease, although mortality in cases of esophageal rupture is very high.
Related Conference: 3rd Euro-Global Infectious Diseases Conferences September 5-6, 2016 Frankfurt, Germany; 3rd Euro-Global Emerging Infectious Diseases Conferences September 5-6, 2016 Frankfurt, Germany; 2nd International Congress on Rare Diseases and Orphan Drugs, October 16-18, 2017 San Antonio, USA; International Conference on Pulmonary Disorders, April 20-21, 2017 Las Vegas, USA; 5th International Congress on Bacteriology and Infectious Diseases May 25-26, 2017 Chicago, USA; 4th Euro Global Conference on Infectious Diseases, October 16-18, 2017 Paris, France; 2nd International Conference on Respiratory and Pulmonary Medicine, August 6-8, 2017 London, UK; 8th International Workshop on Pulmonary Functional Imaging 24–26 March 2017 Seoul, Korea; 58th Annual Meeting of the Japan Lung Cancer Society 4–15 October 2017, Japan; Australian & New Zealand Society of Cardiac & Thoracic Surgeons Annual Scientific Meeting, 6–9 November 2016 Queensland, Australia; International Conference on American Thoracic Society, May 19-24, 2017, USA; Malaysian Thoracic Society Annual Congress, 28–30 July 2016 Hyogo, Japan
Track 8: Epidemiology of COPD
Chronic obstructive pulmonary disease (COPD) refers to a collection of lung diseases that can lead to blocked airways. People with COPD can be at risk for some serious complications that can not only put their health in jeopardy, but can also fatal. In COPD patients, Pneumonia occurs when bacteria enter the lungs, creating an infection. For COPD patients, pneumonia can weaken the lungs. This can lead to a chain reaction of illnesses that can weaken the lungs even further. This downward spiral can lead to a rapid deterioration of health in COPD patients. Respiratory Insufficiency is an important complication of chronic obstructive pulmonary disease. This may represent deterioration in the patient's premorbid condition such that hypoxemia worsens and hypercapnia develops during a relatively trivial respiratory tract infection, which may be viral or bacterial, Alternatively, these changes may occur for the first time in someone with less severe COPD who encounters a particularly dramatic cause for deterioration, e.g. lobar pneumonia or acute pulmonary oedema. Pneumothorax is defined as the accumulation of air or gas in the space between the lung and the chest wall. Also known as a collapsed lung, pneumothorax occurs when a hole develops in the lung that allows air to escape in the space around the lung, causing the lungs to partially or completely collapse. People with COPD, are at greater risk for pneumothorax because the structure of their lungs is weak and vulnerable to the spontaneous development of these types of holes. Pneumo mediastinum must be differentiated from spontaneous pneumothorax. Patients may or may not have symptoms, as this is typically a well-tolerated disease, although mortality in cases of esophageal rupture is very high.
Related Conference: 3rd Euro-Global Infectious Diseases Conferences September 5-6, 2016 Frankfurt, Germany; 3rd Euro-Global Emerging Infectious Diseases Conferences September 5-6, 2016 Frankfurt, Germany; 4th Euro Global Conference on Infectious Diseases, October 16-18, 2017 Paris, France; 3rd world Congress on Infectious Disease, August 28-30, Philadelphia, USA; 5th International Congress on Bacteriology and Infectious Diseases May 25-26, 2017 Chicago, USA; 3rd International Conference on Influenza, September 11-13, 2017 Zurich, Switzerland; International Conference on Pulmonary Disorders, April 20-21, 2017 Las Vegas, USA; 58th Annual Meeting of the Japan Lung Cancer Society 4–15 October 2017, Japan; 74th Annual Congress of the American College of Allergy, Asthma & Immunology (ACAAI) Oct 26-30, 2017 Boston, USA; World Sleep 2017 October 6-7, Prague, Czech Republic; International Conference on American Thoracic Society, May 19-24, 2017, USA; Better Breathing Conference Jan 26-28, 2017 Toronto, Canada
Track 10: COPD Therapeutics At Stages
The symptoms of COPD cannot be completely eliminated with treatment and the condition usually worsens over time. However, treatment can control symptoms and can sometimes slow the progression of the disease. Medications that help open the airways, called bronchodilators, are a mainstay of treatment for chronic obstructive pulmonary disease. Bronchodilators help to keep airways open and possibly decrease secretions. Short-acting anticholinergic medication (ipratropium, Atrovent) improves lung function and symptoms. If symptoms are mild and infrequent, short-acting anticholinergic medication may be recommended only when you need it, and Long-acting beta agonists may be recommended if your symptoms are not adequately controlled with other treatments. Glucocorticoids taken in pill form or as an injection are sometimes used for short term treatment but are not generally used long-term because of the risk of side effects. Several such combinations are available including fluticasone proprionate/salmeterol (Advair) and budesonide/formoterol (Symbicort), which are taken twice daily, and fluticasone furoate/vilanterol (Breo), which is taken once daily. People with advanced COPD can have low oxygen levels in the blood. This condition, known as hypoxemia and the oxygen level can be measured with a device placed on the finger or with a blood test (arterial blood gas). Fatal fires have occurred in people attempting to smoke while using oxygen. Unintended weight loss caused by shortness of breath usually occurs in people with more advanced lung disease. Not eating enough can lead to malnutrition, which can make symptoms worse and increase the likelihood of infection. Other treatments for COPD are including Noninvasive ventilatory support (the use of a special mask and breathing machine to improve symptoms), anti-anxiety or anti-depressant medications, or morphine-like medications to reduce shortness of breath.
Related Conference: 3rd Euro-Global Infectious Diseases Conferences September 5-6, 2016 Frankfurt, Germany; 3rd Euro-Global Emerging Infectious Diseases Conferences September 5-6, 2016 Frankfurt, Germany; 2nd International Congress on Rare Diseases and Orphan Drugs, October 16-18, 2017 San Antonio, USA; 5th International Congress on Bacteriology and Infectious Diseases May 25-26, 2017 Chicago, USA; 3rd International Conference on Influenza, September 11-13, 2017 Zurich, Switzerland; 3rd world Congress on Infectious Disease, August 28-30, Philadelphia, USA; 2nd International Conference on Respiratory and Pulmonary Medicine, August 6-8, 2017 London, UK; International Conference on American Thoracic Society, May 19-24, 2017, USA; World Sleep 2017 October 6-7, Prague, Czech Republic; Malaysian Thoracic Society Annual Congress, 28–30 July 2016 Hyogo, Japan; 74th Annual Congress of the American College of Allergy, Asthma & Immunology (ACAAI) Oct 26-30, 2017 Boston, USA; 8th International Workshop on Pulmonary Functional Imaging 24–26 March 2017 Seoul, Korea
Track 11: COPD Exacerbations
An acute exacerbation of COPD is a flare-up or episode when your breathing gets worse than usual and you become sick. It is most often linked to an infection. Exacerbations are often linked to a lung infection that results from a virus or bacteria, like a cold or some other illness. Spending time in smoggy or dirty air can also make your symptoms get worse quickly. Exacerbations Management may be accompanied by increased amount of cough and sputum productions, and a change in appearance of sputum. An abrupt worsening in COPD symptoms may cause rupture of the airways in the lungs, which in turn may cause a spontaneous pneumothorax. Preventing acute exacerbations Management helps to reduce long-term complications. Long-term oxygen therapy, regular monitoring of pulmonary function and referral for pulmonary rehabilitation are often indicated. Influenza and pneumococcal vaccines should be given. Patients who do not respond to standard therapies may benefit from surgery. Pulmonary Rehabilitations a programme of exercise and education for people with long-term lung conditions help to improve your muscle strength, so you can use the oxygen you breathe more efficiently, improve your general fitness and help you to cope better with feeling out of breath and also help you to feel to stronger and fitter, and able to do more PR is about helping you manage your condition better. It is not a cure, but you will feel better and more confident and in control. PR requires your commitment to really work. People who learn about their COPD and treatment plan are better able to recognize symptoms and take appropriate action. However, education is no substitute for regular exercise as part of a pulmonary rehab program.
Related Conference: 3rd Euro-Global Infectious Diseases Conferences September 5-6, 2016 Frankfurt, Germany; 3rd Euro-Global Emerging Infectious Diseases Conferences September 5-6, 2016 Frankfurt, Germany; 3rd International Conference on Influenza, September 11-13, 2017 Zurich, Switzerland; 2nd International Congress on Rare Diseases and Orphan Drugs, October 16-18, 2017 San Antonio, USA; 2nd International Conference on Respiratory and Pulmonary Medicine, August 6-8, 2017 London, UK; International Conference on Pulmonary Disorders, April 20-21, 2017 Las Vegas, USA; 2nd International Conference on Chest, March 24-26, 2017 Melbourne, Australia; Australian & New Zealand Society of Cardiac & Thoracic Surgeons Annual Scientific Meeting, 6–9 November 2016 Queensland, Australia; Better Breathing Conference Jan 26-28, 2017 Toronto, Canada; 58th Annual Meeting of the Japan Lung Cancer Society 4–15 October 2017, Japan; 74th Annual Congress of the American College of Allergy, Asthma & Immunology (ACAAI) Oct 26-30, 2017 Boston, USA; International Conference on American Thoracic Society, May 19-24, 2017, USA
Track 12: Self-Management and Prevention of COPD
Self- Management interventions help patients with chronic obstructive pulmonary disease (COPD) acquire and practise the skills they need to carry out disease-specific medical regimens, guide changes in health behaviour and provide emotional support to enable patients to control their disease. These programmes are based on the presumption that effective modification of behaviour can be attained only if patients’ self-efficacy has been improved. Patients who have enough confidence in their ability to successfully respond to certain events, such as at the time of an exacerbation, can more easily modify and maintain the desired behaviour. The behavioural modification should ultimately result in improved clinical outcomes. COPD self-management programmes have shown positive effects on patients’ quality of life and healthcare use in secondary care settings, but the benefits in general practice are still inconclusive. There are also breathing techniques that can help you get the air you need without working so hard to breathe, Our primary objective was to assess the long term effects of two different modes of COPD disease management—comprehensive self-management and routine monitoring—on quality of life in COPD patients in general practice. As secondary objectives, we assessed the effects on frequency and patients’ management of exacerbations and on self-efficacy.
Related Conference: 3rd Euro-Global Infectious Diseases Conferences September 5-6, 2016 Frankfurt, Germany; 3rd Euro-Global Emerging Infectious Diseases Conferences September 5-6, 2016 Frankfurt, Germany; 3rd world Congress on Infectious Disease, August 28-30, Philadelphia, USA; 4th Euro Global Conference on Infectious Diseases, October 16-18, 2017 Paris, France; 5th International Congress on Bacteriology and Infectious Diseases May 25-26, 2017 Chicago, USA; 2nd International Conference on Chest, March 24-26, 2017 Melbourne, Australia; 2nd International Conference on Respiratory and Pulmonary Medicine, August 6-8, 2017 London, UK ; 74th Annual Congress of the American College of Allergy, Asthma & Immunology (ACAAI) Oct 26-30, 2017 Boston, USA; Australian & New Zealand Society of Cardiac & Thoracic Surgeons Annual Scientific Meeting, 6–9 November 2016 Queensland, Australia; Better Breathing Conference Jan 26-28, 2017 Toronto, Canada; Malaysian Thoracic Society Annual Congress, 28–30 July 2016 Hyogo, Japan; International Conference on American Thoracic Society, May 19-24, 2017, USA



 Juan Eduardo Keymer R.Â
Juan Eduardo Keymer R.  Margaretha Lundin
Margaretha Lundin  Doris Leung
Doris Leung Kyeong-Soo Lee
Kyeong-Soo Lee YongXiao Wang
YongXiao Wang Hiroake Kume
Hiroake Kume Vasileios Andrianopoulos
Vasileios Andrianopoulos  Michał Zieliński
Michał Zieliński  Nobuaki Miyahara
Nobuaki Miyahara Adhikari Mira
Adhikari Mira Amnon P. Ariel
Amnon P. Ariel Ross Vlahos
Ross Vlahos Hyo-seok Seo
Hyo-seok Seo